
Demystifying UHC — The counter narrative

In the run up to Universal Health Coverage Day on December 12, Dr Adithyan GS, Consultant, National Health Mission, Tamil Nadu and Dr Viduthalai Virumbi, Medical Officer, Directorate of Public Health and Preventive Medicine, Tamil Nadu, give an insight on the lessons learnt from UHC implementation in Tamil Nadu through health and wellness centres
Universal Health Coverage (UHC) is the most popular word in the health circle currently with an extensive literature available to explain its theoretical underpinnings. Even though the idea of UHC was well conceived by many nation states including India, the means and ways to reach the last mile beneficiary remains largely inconspicuous.
Among the flagship schemes that were introduced in the last few years by the Government of India, Ayushman Bharat was one among the notable one, and was given a big push by all policy makers at national and state level. Ayushman Bharat consists of two major health initiatives namely, Health and Wellness centres (HWCs) and National Health Protection Scheme (NHPS). Among this, the former is lauded by almost all in the public health circle and is seen as the window of opportunity to strengthen primary healthcare and the path to achieve UHC in India. Health and wellness centres envisage to provide the 12 comprehensive primary healthcare services at health sub-centres through mid-level health providers and primary health centres through existing staff.
This piece of article is purely the lessons from experiential learnings of UHC implementation in the state of Tamil Nadu through the health and wellness centres (UHC-Health Sub Centers and UHC-Primary Health Centers). This paper deals about how the state has conceptualised the UHC and currently being implemented in Tamil Nadu, with the health sub-centre as the cornerstone of all primary healthcare activities. At all levels of care, the key focus is on re-organisation of service delivery for improved population outcomes.
UHC: A perception for convergence and not another vertical
UHC should never be seen as another national vertical programme with a separate set of guidelines for health programmes. UHC may have the indicators for operationalisation, but not to have separate guidelines for existing programmes like TB, leprosy, maternal and child healthcare.
Globally, UHC aims to reduce the out of pocket expenditure, expanded services and coverage. This shall be conceptualised at the local context to converge all health and related activities by establishing a harmonious programme networks to ensure intact forward, backward and lateral linkages. For example, a diabetic patient for getting drug doesn’t need to depend on single facility, single doctor or fixed timings. Instead the patient can get same drug based on his/her convenience at health sub centre, primary health centre, patient support group, mobile medical unit or even at doorsteps through authorised health workers/volunteers. UHC should bring the perception to health systems that the responsibility of ensuring continuum of care (screening, minor ailment treatment, major ailment first aid, referral service, follow up and rehabilitation), lies with themselves.
The idea of UHC can only be achieved if we are able to develop ‘local health systems’ at a decentralised level- at least at the block level with local ownership. The ultimate goal is about democratising and communitising healthcare where an individual’s 80-90 per cent of healthcare needs are provided, managed and followed up at a block level. While selecting the HWCs, the best mode is to follow the block saturation policy i.e. select all the primary care facilities at the block level except the co-located.
While conceptualising UHC through HWCs, the states should not follow any national or global guidelines instinctively; but has to self-conceptualise and contextualise to place it within the state public health architecture without altering much of the existing state policies. While conceptualising the ideas should actually emerge from the community/field learnings and needs rather than a top to bottom approach. The strategies and concepts are dynamic and ever evolving. Ideally, each block should have a strategic plan considering the epidemiologic and demographic burden, health seeking behaviour of the community, human resource for health and other socio-cultural aspects. The major components of the HWCs-whether it is human resource, infrastructure including branding, training, IT systems, medicines and diagnostics should be tailor made for the state’s public health systems. Health Sub Centre (HSC) strengthening should be considered as the cornerstone of UHC implementation, since it is the nearest and first point of contact in the primary care systems.
Major components of UHC: The key lessons
Human resources
Even though, human resource is the key to implementation of any health-related activities, under UHC the notion should be to build a strong and dedicated primary care team at all levels. The perception that HWC can be operationalised only if we deploy a Mid-level Health provider (MLHP) is not true. The MLHP is meant to work with the team of primary care providers (multi-purpose health workers- male/female) and community volunteers (ASHA/Anganwadi workers/SHG network) to provide the expanded range of primary-care services.
The idea is to bring all the available block level human resources from multiple programs (RBSK, MMU etc.) under one umbrella with clear job roles and responsibilities for providing comprehensive primary healthcare services. Each state can have its own strategies in pooling of these human resources and strategically using them in health service delivery. For example pooling and placing lab technicians at Hub (Block level) on 24×7 basis using existing human resource and maximising the service delivery. It is not a HR reduction strategy, but strategise the assured service delivery to manage acute shortage of lab technicians. Hence, the states with human resource gaps can re-organise their service delivery mechanisms to roll out the UHC implementation by optimally utilising the existing human resource capacity and then progressively fill the gaps as and when resources are available.
Another important aspect is the entry qualification for a MLHP. The key aspect of human resource deployment at the sub centre shall be based on the state context. Available and appropriate work force with primary care skills and motivation to work in remote and rural centres shall be the primary criteria of placing the human resource. Retention of human resource at the centre shall be given due importance in placement of the MLHP.
The job roles and responsibilities also shall be clearly laid down — the MLHP does not replace the doctor, but extends their outreach. The objective of HWC is not to produce qualified quacks should be kept in mind. The MLHP should be guided and bound by the Standard Treatment Guidelines. The career pathways of the MLHP shall also be clearly laid down at the initial stage itself.
All the health staff in state, health unit district, block and institutional level will contribute to UHC implementation as per their existing roles and responsibilities. Health staff job chart shall be periodically updated based on the services delivered from HWCs aiming the harmonious implementation of UHC programme. For effective community engagement, a cadre of community work force is pre-requisite (ASHA, SHG members) in UHC implementation. Here, volunteers from organised sector (SHG) is preferred over the institutionalised health workers.
At state level, establishing a dedicated programme management unit for converging the existing healthcare programme resources is also needed for effective co-ordination with the district and block units as well as with other vertical programme units at the state level itself.
One of the major challenge any state should anticipate is getting sustained financial commitment from the state government for the additional human resources for the HWCs since it involves huge recurring investment and activities that are difficult, even impossible, to cancel, close or scale down once rolled out. The first concern of the finance department will be ‘what is the value for money in spending for an additional human resource in primary care’. To counter this, the state has to create strong evidences of ‘functional UHC models at local level’, which can substantiate the fact that primary care strengthening can yield higher health outcomes at lower per capita total health expenditure.
Capacity building
The key aspect of training should be that it has to be a continuous process and focus on improving hands-on-skills of the MLHP for triaging the walk-ins into screening, minor ailment treatment, major ailment first aid, referral, follow-up and rehabilitation services. The training has to be based on the standard treatment guidelines (STGs) developed for the MLHP. This should impart them skills related to management of common symptoms / common illnesses. The do’s and don’ts should also be a part of the STG. The protocols for various conditions (NCD, IMNCI etc.) and programmatic guidelines like NCD services should be incorporated as a part of the STGs. The capacity building should also include imparting administrative skills, team building skills, skills to manage care pathways and referrals, use of information technology systems etc.
The capacity building should be given to the whole primary care team including community volunteers working in providing comprehensive primary healthcare services. The team should also be given regular trainings together to make each other understand their roles and responsibilities and empowering all the members to work as a team. The case study method is an effective approach to sensitise the importance of job-oriented skills rather than teaching them big volumes of theory materials.
Infrastructure
Infrastructure strengthening is a key priority area in UHC, but unnecessary focus on branding can yield negative outcomes and wastage of resources. Since, the major proportion of money from HWC is earmarked for infrastructure strengthening, the funds for the same should be spend towards strengthening of appropriate infrastructure for service delivery. For example, laboratory strengthening, training infrastructure at block should be given priority over the new HSC construction.
The states should initially select sub-centres with reasonably good infrastructure and convert it as HWCs and concomitantly build new constructions through public works department than outsourcing to private enterprises to build branded monuments in place of good quality health centres, where even a poor patient from lower social strata finds hesitant to come. As an interim arrangement for transforming HSCs without government buildings into HWC, Village Panchayat Service Centres (VPSC) building or other government rent free buildings can be utilised. Ownership of the HSC level activities to health staff comes along with health infrastructure for delivering the services.
Patient waiting area covered to accommodate at least 10-15 chairs, citizen charter, designated space for lab/diagnostics, provision of wellness room for Yoga, bio medical waste management, well-ventilated clinic room with examination space and office space for MLHP, rack for storing medicines, equipment, documents, health cards and registers, display boards for Information, Education and Communication (IEC) in local language which also includes assured services and HWC details, assured water supply – Running / Potable, power supply, appropriate backup with solar source, inverter, emergency lamps and solar torch lights, separate male and female toilets, Proper drainage facility, adequate residential facilities for the service providers are essential for a functional HWC.
Additionally, at Primary Health Centres electronic, display boards for IEC and HWC services, space for laboratory and pharmacy, need to be strengthened. At Block Primary Health Centre, CPHC training hall for tele mentoring and dedicated laboratory buildings should be present. The HWCs should also be linked with the quality assurance programme and kayakalp.
Drugs and drug delivery systems
A robust drug and diagnostics systems is a pre-requisite for any UHC model from the financial point of view since the maximum out-of -pocket expenditure for any individual accessing a health facility is towards drugs and diagnostics. The first and foremost aspect in drug component is finalising the drugs to be dispensed through the health and wellness centres, well aligned with STG and displaying it at the HWC. The drugs other than Kit A, Kit B and family welfare kits should be selected with expert committee consultations which must include field level implementers and based on local profile of diseases. The NCD drugs dispensation will be a key factor in success of any UHC implementation due to the prevailing epidemiologic and demographic transition across almost all states in the country. Additional consumables and surgicals are also to be made available to provide the CPHC services under UHC. In view of bringing clarity to health staff involved in CPHC service delivery, drafting the process of each activities related to service delivery, drugs and diagnostics requirement, meeting demand and supply at HWC level have to be decided at state level before implementing the UHC.
In view of preventing antimicrobial resistance, rational use of antibiotics is strategically restricted by advisory stating that antibiotics should only be used as per IMNCI, SBA, Sepsis and other State/Nation approved protocols. Health staff should be oriented to ensure the completion of antibiotic course initiated at all levels.
Every UHC HSCs should be issued a separate drug passbook which has to be maintained by the MLHP. This should be included as a job role of the MLHP. The drug inventory should be made as a part of the Health Information Technology Systems (HITS). This will be the sustainable solution to track procurement and adequate supply, drug usage, avoid wastage, proper redistribution of drugs etc. There should also be a proper mechanism for safe storage, transport and redistribution of drugs. Drug utilisation should be generated from the line list of walk-ins availed services at HWC.
Diagnostics systems
The diagnostic systems are as important as drug delivery systems. The number of diagnostics tests available at each level of primary care should be arrived at first instance, which depends upon lab technician availability, diagnostics and reagent availability, infrastructure status etc. Since lab technician availability is a perennial problem in many parts of the State, the ideal model is to roll out Hub and Spoke model of laboratory services with Lab Information Management Systems (LIMS). This is also the most efficient system from patient’s point of view since it cut downs indirect costs as well. Tamil Nadu has fixed five lab tests to be done at HSCs, 20 lab tests at PHCs, five additional tests at CHCs, 11 tests at District Public Health Lab (DPHL) and four tests under insurance (CMCHIS) through the ‘HUB and Spoke’ model.
The major aim is to provide the basic investigations at HWC and refer samples instead of patients for higher investigations. Transportation support has been arranged through bike and available means in the local area. The major challenge here will be the operationalisation aspect i.e. to institutionalise the sample transport mechanisms. A ‘One size fits all’ may not work here ・the need of local systems at each block/district level based on the terrain, availability of human resource etc. should be arrived for effective implementation.
Finally, the hub and spoke model should be extended and integrated to government hospitals and medical college hospitals for provided essential diagnostic services with expanded list of test menu. The success of an efficient drug and diagnostics systems will be a key determining factor for the success of any UHC models.
Mere provision of drug allocation, supply chain management system, diagnostic equipment, consumables, hub and spoke transportation support and lab technicians will never work unless the networking and process is insured on daily basis. The health system should aim to provide the drugs and diagnostic service on 24×7 basis to gain the confidence of public who unknowingly spend money towards seeking healthcare at least in identified strategically located HWCs.
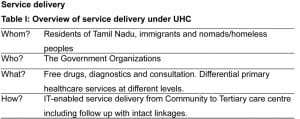
UHC is not provision of universal set of services at health sub centre, but it’s about provision of differential services at differential level of health systems. This should not be read as provision of selective packages of services. Under UHC, the patient should have choice to avail services at any convenient point of service delivery without any cost of care.
The service delivery has to be conceptualised in such a way that the primary care team with MLHP, supported by the supporting staff does the early detection, the medical team establishes diagnosis and treatment plan, and the primary care team supported by community volunteers (ASHA/Women Health Volunteer/SHG network), patient groups ensures follow up and medication compliance.
The state which is currently going through the epidemiologic transition has conceptualised expanded service delivery with focus on NCD services without compromising MCH services and communicable disease management. Patient-centric convergence of all existing health and related activities at block level is what the state is aspiring for under the UHC programme.
In many states, the MLHP’s role is conceptualised as a healthcare provider, providing diagnosis and treatment for a wide variety of illnesses- going beyond the RCH range. The focus now is just on increasing footfalls in what is described as a general OPD. This is also setting a wrong precedence and diluting the service delivery aspect to mere numbers. The thought of enumerating complete population and creating a starting point for service delivery is quite inappropriate in highly dynamic population. The ultimate focus should be on population-based outcomes rather than counting footfalls. Health promotion activities, addressing social determinants should also be considered as an important component and are to be built into the programme, usually as community-based response to high incidence of related diseases/risk factors in the community.
One of the challenges of operationalising HWCs is the integration of hitherto vertical disease control programmes viz-control of TB, HIV, vector-borne diseases, leprosy and blindness into primary health care programmes. Under UHC, the focus should be on provision of integrated services at four levels: the family or the community level, at the service delivery level (health and wellness centre), convergence level (block) and the first referral unit.
The following aspects are key in improving service delivery under UHC:
- Standard Treatment Guideline (STG) for VHN and Staff Nurse for providing the Primary Healthcare Services
- Hands-on training at Block level for service provision and IT systems
- Linkages of CPHC services from community to First Referral Unit
- Clear job responsibility of public healthcare team
- Effective IEC strategies through local innovations
- Ensuring adequate drug availability and indenting from the level of Sub centre
- Hub and spoke model to maximise the lab support to HWCs
- Building mentoring teams and motivated local leadership among healthcare providers at Block Level for Clinical Audit and regular monitoring
- Changing the reporting pattern from raw numbers to line lists and sharing it at all levels up to the community volunteer (can start with NCDs, TB, High risk mother etc.)
- Reinstating community’s faith in public health systems through community engagement in service delivery
Community engagement
Health system has lost its community linkages like coordination with ICDS, direct cash benefit over MCH outreach, immunisation target over programme target. Outreach service under UHC is the re-entry to community to reinstate the faith in public health care systems of community. Community-based palliative and geriatric care, NCD follow up may be the initial focus of outreach. Establishing the linkage between Institutional services and outreach activities like MCH services, immunisation, family welfare services, Hospital on Wheels (HoWP), School Health (RBSK) Team will throw light on the path to UHC. The concept of UHC has to be kept open for accepting the feedback and evolve over the time within healthcare systems.
Population-based screening of NCDs and specific communicable diseases including enumeration of beneficiaries by house to house visit, screening for 18-29 for NCD risk factors using Community-Based Assessment Checklist (CBAC), Screen for 30 and above for diabetes, hypertension, cervical, breast and oral cancers (blood sugar and blood pressure), Symptomatic screening of TB, leprosy, Mental health, COPD & CKD through Woman Health Volunteers (WHV)/ASHA/AWW) are the new value addition under UHC programme in Tamil Nadu. Understanding the field reality and tailor made guidelines for each programme will help in improved service delivery and bring health staff together ensuring the readiness for programme convergence.
Organising meetings at HSCs with the community to showcasing the HSC services, Self Help Group (SHG) meeting and Village Health Sanitation & Nutrition Committee (VHSNC) meetings, Organising School Children for HSC visits (Schools located within the village only), conducting Village Health Nutrition Day regularly at the HSC in coordination with ICDS, Community Partners meeting, regular meetings with mothers and NCD patients (patients support groups), district/block health assemblies, inviting all govt/local body staff working/residing in the village to the HSC for sensitisation on expanded service delivery at HWCs are few strategies which will strengthen community engagement. The vision is to create HSCs as epicentre for major activities in the community.
All the community action from health department should collaborate with the guidance of the gram panchayat and the local community to take action on environmental and social determinants. This can be made more vibrant under the Community Action for Health (CAH) programme which should also be integrated with the UHC programme.
The HWC has the potential to communitise and democratise healthcare, provided the community engagement is robust. When a volunteer reaches the community, the person will be able to get follow up details of each affected/diseased individual from both the government and private beneficiaries. The sustainability quotient of UHC solely depends on demand creation among the local community. In the absence of good community models, the outcomes of most NCD control programmes can be very poor. Patient support group formation is a way forward, since the health institution models by itself can’t achieve the desired follow up rates for care going by the long standing experience of Government of Tamil Nadu in facility based NCD management.
Information technology
All current health applications are currently focussed on getting the footfalls i.e. numerator. The state has conceptualised that the Comprehensive Universal Health Coverage IT platform with population as denominator is essential to establish a continuum of care from community to referral units. As a first step, Health IT standards was drafted. Family folders module, outpatient module and drug inventory module were developed using the standards.
Conceptualisation of UHC IT Platform
The following are the key conceptualisation points while developing Universal Health Coverage Information Technology (UHC IT) Platform in Tamil Nadu
- Master Registry (denominator): A common list of health facilities, service area mapping, family folders with unique identifier
- Offline capability, quick search, local language, near real-time data exchange, cross-platform usage
- Longitudinal personal/public health record for continuum of care
- Intact forward and backward referral mechanism, within and between the health applications and from community to tertiary care facility
- Aligned with state, national and global health data requirements
- Portal for public communication
- Digital cohort of the state with Data Cooperative Model (DCM)
- Interactive dashboard for evidence based decision making with GIS, AI/ML
- Compliance Health IT standards, IT Systems and security standards
- State-owned platform for IT-enabled health service delivery
6.6 crore individuals as 2.05 crores families are mapped with 13,640 hospitals across 2.03 geographical units with GIS-based organisational hierarchy levels. This common database with unique identifier is pivotal in linking the programme data and converting data points into digital cohort. Robust IT Systems with master registry is required to support intact forward, backward and lateral linkages from community to tertiary care centres. State should think of linking the births and deaths into the master registry to keep it alive. All health facility and community extensions should take the responsibility to update the datasets periodically or as and when they come to know at the earliest.
IT systems approach
UHC IT Platform approaches the users as systems approach which is the environment where users will interact with the IT Platform. The following major components are given priority
- Hardware: Laptop, Tablet-PC, desktops
- Software: Applications and credentials
- Internet Connectivity and networking: sustained internet in all health facilities
- Hands-on training: Block level training given to VHN/SN/ANM
- Mentoring and supervision: Daily performance audit and clinical audit
The block, district and state level teams has been oriented through Training of Trainers (ToT) on IT systems gap analysis. Offline usage of application and quick search of patient details were the two major feedback received during the ToTs. The provision of IT systems has to be ensured at local levels, maintenance over time, logistics, roles and responsibilities bring the dream to reality. Users at all levels are in need of platform with cross platform capability, so investing in devices may be restricted to which are used by field staff. Instead of forcing them to use tablets which is less powerful in the same price range. Assured Internet connectivity provision to all health staff is identified as bottleneck in implementing the UHC IT Platform.
The state has started activities for establishing elastic search facility and offline packaging of the existing online application with eight modules in a phased manner. IT systems evolution at global level like quantum computing, artificial intelligence should never be a mandate for the health system change. Instead the Health IT architecture should be flexible and robust enough for horizontal (programmes), vertical (organization levels) and lateral (inter department) expansion. The learnings from the state is that appropriate use of Health Information Technology systems would support service delivery under UHC but would never be a substitute for them and the programme convergence should precede before IT convergence.
Role of development partners
The role of civil society organisation and other development partners are crucial in success of UHC programme. The government should take this step cautiously when it comes to selection of development partners-both for funding as well as technical inputs from private sector. Think tanks may be established by empanelling subject matter experts. Government has to periodically review the progress of programme and contributions from these think tanks.
Even though we completely agree with the fact that anyone not functioning in public can’t be labelled as private, most of the NGOs and research organisations working as development partner for various state governments are funded by philanthropic capitalists who lacks the critical understanding of the public health systems objectives and moreover the local contexts. Most of these organisations ulterior motive is not to catalyse social transformation or improvement of public health systems but as mere instruments of a funder trying to meet a goal. But, the collaboration with other government departments and agencies (Panchayati Raj, Rural/Urban Development, Women Development, Education etc) is quintessential for the success of any UHC models.
The various state governments who are striving towards achieving universal healthcare to all its citizens should clearly understand the fact that only a public funded and owned UHC model will work sustainably in the long run, even though with all its deficiencies and defects. Hence, the development partners impersonating the hard work of public health systems should be dealt vigilantly. All the developments and guidelines should be owned by the public systems (source codes, datasets, copyrights, intellectual property rights). States should get the stack from the outcomes of implementing the IT platform and not seen as agency for data collection.
Major challenges foreseen during implementation of UHC
The following challenges may be considered during implementation of UHC
- Upscaling UHC programme to entire state in a short span by the unrealistic timelines set up
- Sensitising the health staff on operationalising the HWCs to provide CPHC services i.e. from selective care to comprehensiveness
- Shortage of trained manpower to deliver the 12 CPHC services
- Training of health staff on job-oriented syllabus and career progression advantages of trained staff.
- Strengthening the community linkages
- Moving from paper-based registers to IT-based systems
- Generating population enumeration line list: Fixing the denominator
- Functional Lab Information Systems (LIS) and Hub & Spoke model
- Convergence of established programmes like NCD, MCH services, Family Planning services, RBSK, Urban polyclinics under UHC
- Political and financial requirements and commitments.
Conclusion
Experiential learnings of health systems, readiness for implementing the UHC programme and financial support from Government of India made the conceptualisation acceptable to health staff and administrators in context of Tamil Nadu. The states should capitalise UHC as an opportunity to strengthen the primary healthcare machinery through public systems strengthening but not at the cost of secondary and tertiary care facilities, which is also required to complement the primary care systems.
Tamil Nadu’s experience has proved that strategic purchasing of healthcare from private sector either through Insurance or Public Private Partnership (PPP) mode without the presence of a strong and robust government sector is a recipe for disaster, and will be unviable in the long run. The states should strive for creating their own local models and try to build each components under UHC through in-house models rather than outsourcing/PPP modes, which has its own moral hazards and sustainability and equity issues.
The paper stems from the field learnings during the UHC implementation in Tamil Nadu through HWCs. The major learning was that each field visit during the implementation phase gave new insights and conceptual clarity regarding the concept of UHC. The major challenge in implementation is also the same- i.e. the concept is dynamic and various local health systems perceives it in different ways. The only concluding point is that each state government should conceptualise and place the UHC concept within its local health systems rather than fixing borders for the UHC cube.
(The views the authors express in this opinion pieces are entirely their own and from the experiential learning from field level implementation of the UHC program in Tamil Nadu)
- Advertisement -